Exposure Response Prevention (EPR) for OCD
Dr. Jen Viscusi is a licensed psychologist specializing in OCD and Exposure and Response Prevention (ERP) therapy. She provides evidence-based OCD treatment for adults across New York, with telehealth statewide and in-person sessions in NYC.
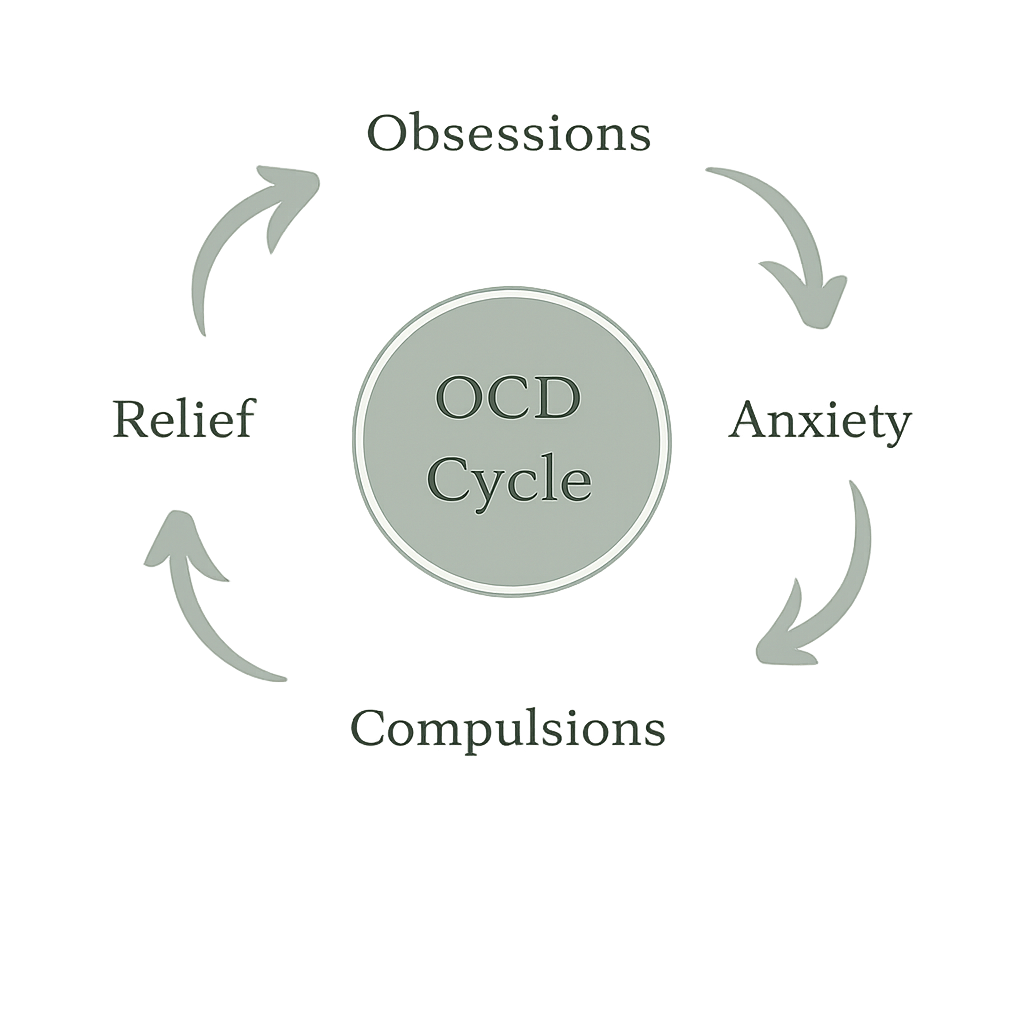
ERP is a structured behavioral treatment for obsessive-compulsive disorder. It works by helping you deliberately approach triggers (thoughts, images, sensations, situations) while practicing a different response: no compulsions, no reassurance, no avoidance rituals. Over repeated practice, the OCD cycle weakens and you build durable tolerance for uncertainty.
ERP is not insight-based therapy for OCD. It is skill-based training: planned, measurable, and designed to create behavioral change.
On This Page:
What ERP Is
Exposure and Response Prevention (ERP), sometimes written EX/RP, is a specialized behavioral treatment for OCD that sits within, but is distinct from, general cognitive-behavioral therapy (CBT) approaches. While CBT is a broad therapeutic framework, ERP is the first-line, evidence-based treatment specifically shown to address the mechanisms that maintain OCD.
The “exposure” portion involves intentionally contacting triggers that evoke obsessions or distress. The “response prevention” portion involves choosing not to do the behaviors or mental acts that OCD demands in order to feel certain, safe, or “back to normal.”
ERP targets the engine of OCD: short-term relief strategies (compulsions and avoidance) that keep the disorder running.
How ERP Works
(Mechanism, Not Motivation)
ERP is based on decades of research in learning theory and behavioral neuroscience, demonstrating that repeated exposure to feared triggers—paired with the prevention of compulsive responses—leads to durable changes in how the brain processes threat, uncertainty, and discomfort.
Exposure
Exposure means purposely bringing on the obsessional trigger in a planned way. This can include:
real-life exposures (in-vivo)
imaginal exposures (for feared outcomes you can’t “test” directly)
interoceptive exposures (to bodily sensations)
practice with triggering words/images/ideas when relevant
Exposure is graded and strategic. The goal is not to proove a thought is false. The goal is to practice living well while uncertainty remains.
Response Prevention
Response prevention means learning to drop the actions OCD uses to manage distress, including:
overt rituals (checking, washing, repeating, confession, reviewing, seeking reassurance)
avoidance and safety behaviors
mental rituals (silent neutralizing, undoing, mental checking, “figuring it out,” internal reassurance)
Response prevention is where the treatment happens. Without it, exposure becomes another way to “get certainty.”
What changes over time
As you practice, several shifts typically occur:
triggers become less “sticky,” less controlling
urgency to ritualize decreases
your ability to tolerate uncertainty increases
you learn you can function while discomfort is present
OCD’s rules lose authority
This is not willpower. It’s learning through repeated corrective experience.
What ERP Looks Like in Practice
Assessment and case formulation
We start by clarifying:
your obsession themes, compulsions, avoidance patterns, and safety behaviors
how OCD is maintained in your specific case
the difference between reasonable caution and OCD rules
what “treatment targets” matter most in daily life
Build the exposure plan
ERP is not random bravery. We build a structured plan that includes:
a hierarchy (graded difficulty)
response-prevention rules that are specific and trackable
“drop the ritual” strategies for both behaviors and mental compulsions
practice targets that map onto your real life (not hypothetical scenarios)
In-session work + between-session practice
ERP works best when it becomes a practice, not a weekly discussion.
Sessions are active: planning, exposures, and coaching your response prevention.
Between sessions you complete structured practice assignments.
We review outcomes, refine targets, and adjust pacing based on data—not mood.
Measurement and course-correction
We track progress in practical terms:
time spent ritualizing
avoidance reduced
decisions made without checking/reassurance
reclaiming activities that OCD has restricted
When something isn’t moving, we troubleshoot the mechanism (often hidden rituals, subtle avoidance, or reassurance loops).
Common Misconceptions (What ERP is Not)
ERP is not flooding. It should be titrated, strategic, and clinically guided.
ERP is not “just do the thing and white-knuckle it.” You’re learning specific response-prevention skills.
ERP is not reassurance. A therapist’s job is not to make OCD feel certain.
ERP is not about proving thoughts are irrational. It’s about changing your relationship to uncertainty and compulsion.
ERP is not generic talk therapy for anxiety. OCD has a distinct reinforcement loop that must be treated directly.
Who ERP Is a Good Fit For
ERP is a good fit when you:
are willing to examine compulsions/avoidance as part of the problem (even if they feel necessary)
are willing to practice between sessions
want a structured approach with measurable targets
are ready to change behaviors, not just understand them
prefer a treatment frame that is direct, skills-based, and accountability-oriented
You do not need to feel confident to start. Many people begin skeptical or anxious about ERP and still do very well with a clear plan.
When ERP May Not Be The Right Starting Point
ERP may not be the first step when there is:
acute instability that prevents consistent practice (e.g., severe depression with inability to function, active substance dependence)
unmanaged risk requiring stabilization first
circumstances where additional stabilization or supports are needed before beginning ERP.
In those cases, the plan is usually stabilize first, then do ERP, not avoid ERP indefinitely.
ERP With Me
My clinical focus
I am a licensed clinical psychologist with specialized focus in OCD treatment using ERP. My work is designed to be precise, structured, and clinically grounded, especially for presentations that are easy to miss or mis-treat (including taboo intrusive thoughts and high shame themes).
Format, pacing, and expectations
Work with me typically includes:
a clear formulation of your OCD cycle
a tailored exposure plan that targets your rituals and avoidance
in-session coaching and deliberate between-session practice
steady refinement to prevent ERP from turning into reassurance or “perfect practice”
ERP requires effort. My job is to make that effort well-aimed.
Private-pay and fit
I’m private-pay and specialization-driven. That is intentional, as ERP is a technical treatment, and outcomes depend heavily on clinical skill, structure, and follow-through. I work best with people who want a focused, active treatment process and are ready to practice. (If you’re unsure, that’s fine; we clarify fit early.)
Evidence Base and Clinical Standards
ERP is widely recognized as a first-line, evidence-based treatment for OCD and is recommended by major clinical and public-health bodies.
The following sources reflect established clinical standards and consensus recommendations:
Frequently Asked Questions
-
Yes. ERP is highly effective for OCD with mental or internal compulsions (sometimes called “Pure O”). Treatment focuses on reducing rumination, reassurance, and other covert rituals while helping you build skills for uncertainty. I work with many individuals experiencing primarily mental compulsions using structured, evidence-based ERP.
-
No. ERP is always collaborative and paced appropriately. We build exposures gradually based on your readiness, not by forcing overwhelming situations. The goal is to help you face fears in a way that feels challenging but manageable, so you can build confidence over time.
-
Not as a primary mechanism. ERP is a behavioral, skills-based treatment focused on changing how you respond to intrusive thoughts, not analyzing their origin. While understanding your experiences can be helpful, ERP is designed to create real-time change in how OCD operates day-to-day.
-
The length of ERP varies depending on symptom severity and consistency of practice, but many people begin to see meaningful improvement within a few months. ERP is designed to be structured and goal-oriented, with a focus on building lasting skills rather than ongoing open-ended therapy.
-
That is completely reasonable and you are not alone. I offer a consultation where we can discuss your symptoms, how ERP would apply to your situation, and what treatment would look like. This gives you a clear sense of the approach before deciding whether to move forward. You can also read anonymous reflections from clients who completed ERP with me on my ERP Experience page.